
18
Feb
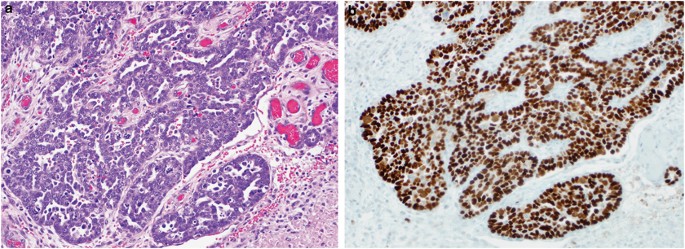
Diffuse positive overexpression 97 and diffuse negative complete absence. Aberrant p53 expression detected by immunohistochemistry has been known to be a surrogate marker of TP53 mutation in ovarian serous carcinoma.
P53 negative serous carcinoma. Using an illustrative case study and a review of the literature we explore a relatively routine diagnostic question. Whether the negative predictive value of a wild-type p53 immunophenotype for serous carcinoma is absolute that is whether a p53-wild type immunophenotype is absolutely incompatible with a diagnosis of serous carcinoma. The case is an advanced stage endometrial.
Strong and diffuse immunoexpression of p53 is generally interpreted as likely indicating a TP53 gene mutation. The immunoprofile that correlates with wild-type TP53 however is not as clear. In particular the significance of completely negative immunostaining is controversial.
The aim of this study was to clarify the relationship of the immunohistochemical expression of p53 with the mutational status of the TP53 gene in ovarian cancer. A total of 57 ovarian carcinomas. The tumor cells are positive for CK7 and PAX8 with abnormal overexpression of p53 but negative for CK20.
Estrogen receptor and progesterone receptor expression is negative. These features are best characterized as high grade serous carcinoma which displays a SET solid pseudoendometrioid or transitional pattern. Ovarian carcinomas which show a SET pattern of high grade serous carcinoma.
Most serous carcinomas exhibit aberrant p53 expression while this is only seen in up to a third of clear cell carcinomas. Serous carcinomas are typically negative for Napsin-A and AMACR whereas the majority of clear cell carcinomas are positive for these markers at least focally. Moreover a small number of serous carcinomas are p53 negative and some are positive for ER and PR.
Additionally mixed serous and endometrioid adenocarcinomas are not uncommon and these also may have an overlapping immunophenotype. The tumour suppressor p53 is mutated in cancer including over 96 of high-grade serous ovarian cancer HGSOC. Historically p53 IHC has been interpreted as negative or positive based on the percentage of stained tumor cell nuclei using variable cut-offs which range from 5 to 50.
Uterine papillary serous adenocarcinomas showed significantly higher p53 overexpression than uterine endometrioid adenocarcinomas 1000 versus 610 p. Nuclear overexpression of p53 whereas six tumors 15 were p53 negative. Thirteen p53-positive tumors had multiple samplings from distinct anatomic sites and all showed complete concordance in p53 staining suggesting that p53 alterations occur early in UPSC.
Aberrant p53 expression detected by immunohistochemistry has been known to be a surrogate marker of TP53 mutation in ovarian serous carcinoma. 96 Aberrant p53 expression is mainly divided into 2 distinctive patterns. Diffuse positive overexpression 97 and diffuse negative complete absence.
98 The diffuse p53 positivity and negativity are believed to be associated with gain-of-function and loss-of. Although p53 signature benign-appearing epithelial cells with p53 diffuse expression is frequently found in the fallopian tubes the clinical and pathological significance of this lesion in the case of high-grade serous carcinoma HGSC patients still remains unclear. A wild-type pattern of p53 expression ie p53 staining in scattered nuclei of tumor cells is typical of papillary ECa of intermediate grade while serous carcinoma is characterized by aberrant.
High grade serous ovarian cancer is characterised by high initial response to chemotherapy but poor outcome in the long term due to acquired resistance. One of the main genetic features of this disease is TP53 mutation. The majority of TP53 mutated tumors harbor missense mutations in this gene correlated with p53 accumulation.
TP53 null tumors constitute a specific subgroup characterised by. Serous EIC showing aberrant pattern of p53 expression The histologic differential diagnosis includes papillary syncytial metaplasia PSM with degenerative atypia 56 58 radiation-associated atypia or metastases. Positivity for p53 was strong and diffuse 100 of tumor cells in 5 uterine tumors and in 3 ovarian tumors.
P53 expression in 6 of the uterine specimens and 7 of the ovarian specimens was present in fewer tumor cells of weak intensity or both. TP53 mutations are ubiquitous in highgrade serous ovarian carcinomas HGSOC and the presence of TP53 mutation discriminates between high and lowgrade serous carcinomas and is now an important biomarker for clinical trials targeting mutant p53. P53 immunohistochemistry IHC is widely used as a surrogate for TP53 mutation but its accuracy has not been established.
MAPK positive staining was detected in 636 of low-grade Figure Figure1B1B as opposed to 171 of high-grade carcinomas. The high-grade group is represented with 829 of MAPK negative carcinomas Figure Figure2B2B. Ten out of 70 143 high-grade samples showed simultaneous p53 and MAPK immunoexpression.
Most originate in fallopian tube. Normal tube P53 mutation Serous tubal intraepithelial carcinoma STIC Invasive High-grade serous carcinoma of tube spreads to ovary Essentially tubal origin until proven otherwise. Only consider primary ovarian if both tubes are completely histologically examined and free of disease.
If both tubes and ovaries negativeprimary.
Previous post
Pain catastrophizing scale score interpretationNext post
P acnes gram stain